

The CDC just hid information about a biological weapon featured in "Epidemic of Fraud"
Since I referenced Q-Fever in "Epidemic of Fraud", the CDC deleted some info about a bacteria Coxiella Burnetti, including a section called 'Considerations for intentional release'.
In emails to Janet Woodcock featured in “Epidemic of Fraud”, we discussed a biological weapon known as Coxiella Burnetti, aka “Q Fever”. Coxiella infection in humans has many of the same symptoms we were told was COVID-19 in 2020.
According to the ‘old’ CDC page, these are the signs and symptoms of Coxiella infection.
Q fever can cause acute or chronic illness, and people are commonly exposed from contact with infected animals or exposure to contaminated environments. The acute symptoms usually develop within 2-3 weeks of exposure, although as many as half of infected people are asymptomatic.
The following is a list of symptoms commonly seen with acute Q fever. However, it is important to note that the combination of signs and symptoms vary greatly from person to person.
High fever (up to 105°F)
Fatigue
Severe headache
General malaise
Myalgia
Chills or sweats
Non-productive cough
Nausea
Vomiting
Diarrhea
Abdominal pain
Chest pain
Most people with acute Q fever infection recover completely; however, some may experience serious illness with pneumonia, granulomatous hepatitis, myocarditis, or central nervous system complications.
The CDC has now changed the website to hide some information. Especially anything regarding the WHO. Both old and new versions encourage humans to avoid interacting with animals and drinking raw milk. Remember when meatpacking facilities were major sources of outbreaks for COVID? That would be a significant way to spread Q Fever too! The CDC was also aware of the risk.


In fact, in 1986 the CDC investigated Q Fever in slaughterhouse workers and discovered a high number of them tested positive for Q Fever exposure! Nothing to see here!
A serosurvey was conducted to identify the extent of the outbreak. Forty-two of approximately 100 employees agreed to be surveyed, including the five employees described above. Twelve (29%) had complement-fixation (CF) titers to Q fever rickettsiae; eight (67%) of the 12 had recently experienced a clinical illness compatible with Q fever. Nineteen (45%) of the surveyed employees were positive by IFA test (but negative by CF test) for IgG antibody. Eleven of the 42 employees were negative both by CF and IFA. The 31 persons with serologic evidence of infection worked in a variety of jobs in areas throughout the plant, but no further investigation was performed to determine areas of highest risk.
Both Q Fever and COVID also had unproductive coughs, extremely high fevers, severe headaches, and stomach flu symptoms. Q Fever is also linked to myocarditis, something we are seeing in unprecedented numbers across the United States.
PROJECT CD-22 - US Army Q Fever Experiments
Remember our secretive friend Eric O. Freed at the National Cancer Institute at Fort Detrick? Guess what! His home base also conducted experiments on humans with Q Fever. It’s how we know how to weaponize this highly contagious airborne bacteria.
Operation Whitecoat volunteers largely consisted of Seventh-Day Adventist draftees, who were trained as medics but whose religious convictions forbade combat. Approximately 2300 individuals participated in the program. The Army completed about 150 studies during the Operation Whitecoat years. Experimenters exposed volunteers to disease-causing agents such as Q fever and tularemia under strict protocols to study immunity to disease and to conduct drug therapy. Whitecoat volunteers also participated in safety studies of vaccines designed for protection against Venezuelan equine encephalitis, Eastern and Western equine encephalitis, plague, tularemia, Q fever, yellow fever, chikungunya virus and Rift Valley fever. There were no fatalities or long-term injuries among Whitecoat volunteers. The program ended in 1973 upon termination of the military draft.

What did the CDC change two weeks ago?
The entire layout of the Q Fever site has been overhauled to be simpler. Especially a very important section under a tab labeled ‘For Healthcare Professionals’ title “Considerations for Intentional Release”.

I’m including a screen grab as well as a text copy of this very important information.
Considerations for Intentional Release
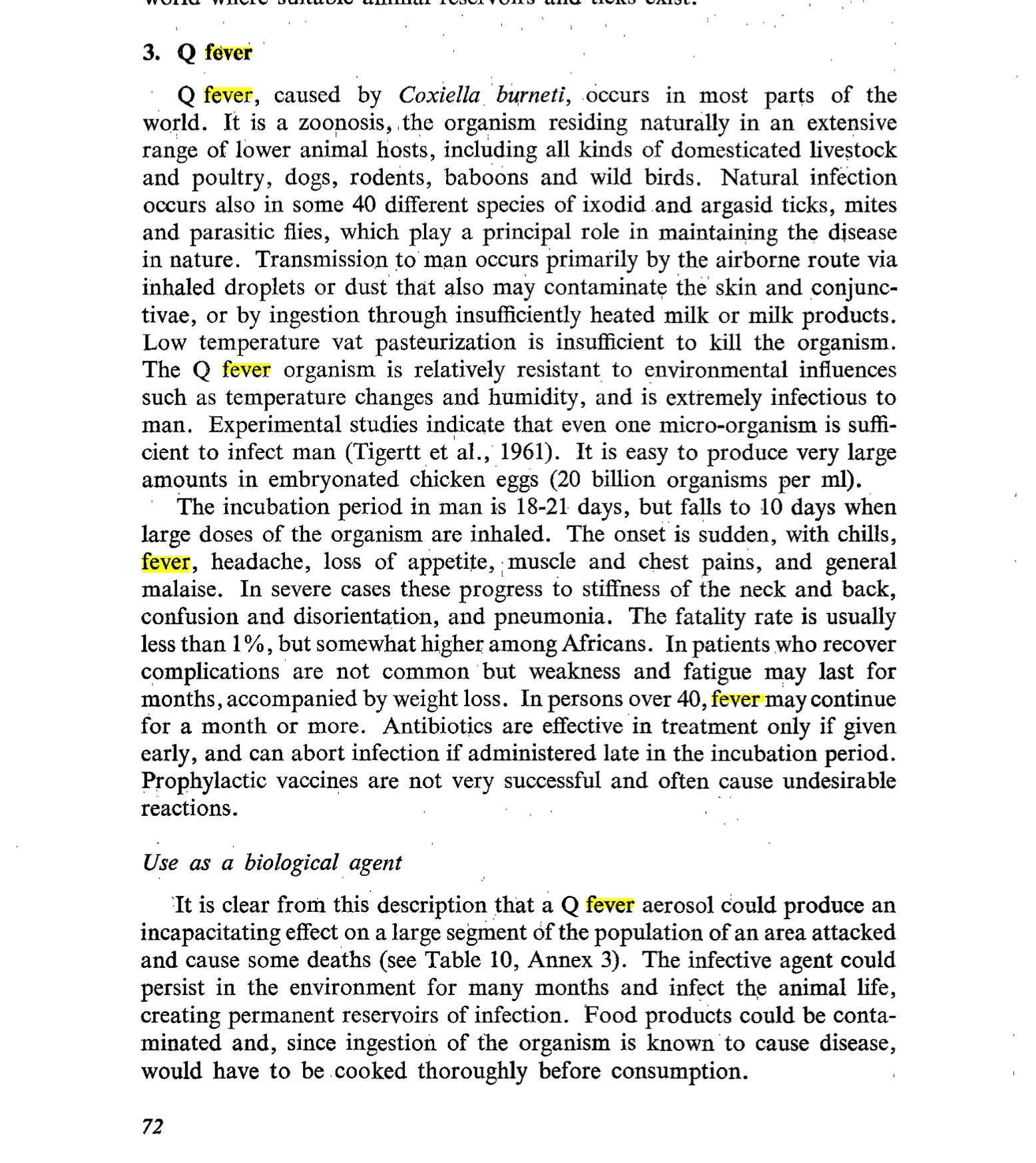
C. burnetii is a highly infectious agent that is resistant to heat, drying, and many common disinfectants.
It can be aerosolized and inhalation is the primary route of infection for people.
As few as 1-10 C. burnetii organisms may cause disease in a susceptible person.
This agent has been previously weaponized for use in biological warfare and is considered a potential terrorist threat.
The World Health Organization has estimated that if 50 kg of C. burnetii were aerosolized over an urban area with 500,000 inhabitants, there would be 125,000 cases of acute illness, 9,000 cases of chronic Q fever, and 150 fatalities (Health aspects of chemical and biological weapons, 1st edition, 1970external icon).
Person to person transmission is possible via transplacental exposure, sexual contact, blood transfusion, and transplantation.
Nosocomial infections have been rarely reported following autopsies and obstetrical procedures involving infected persons. (For more information on Occupational Exposure and Prevention relating to Q fever see the CDC’s MMWR Diagnosis and Management of Q fever—United States, 2013)
Clusters of pneumonia, or unusual clusters of acute febrile illness with respiratory involvement or granulomatous hepatitis, in a community where no other cause can be identified may indicate a possible intentional release of C. burnetii.
In cases of suspected intentional release, post exposure prophylaxis (doxycycline 100 mg twice a day for 5-7 days) can be considered in groups determined to be at high risk for exposure, but is not recommended for the prevention of naturally occurring Q fever. Chemoprophylaxis is only considered effective if administered within 8-12 days of exposure.
The WHO link the CDC provided is curious because it has not been functional for several years. The CDC page even links to an archive page that is also unavailable. Here is the information on a working version of the WHO page that discusses how much weaponized Coxiella to spray over an urban area.
We had to dig to find the original document the WHO links to. Here’s the WHO link.
Here’s a backup of the original document in case the WHO pulls a CDC and disappears the information.
So what does the new CDC page say?
The new CDC page acknowledges the bioweapons history of Coxiella but leaves out quite a bit of other information, including anything about the World Health Organization. I wonder why?
The treatment for Coxiella is Hydroxychloroquine and Doxycycline.
If you recall, we had a discussion with Didier Roult who was ecstatic after seeing Epidemic of Fraud. Pr Roult pointed out that Janet Woodcock refused to discuss Coxiella with us because she would have had to admit that his 30 year old protocol for Q Fever was HCQ/Doxycycline was safe in higher than average doses of HCQ. Even at higher doses, the HCQ was still safe for patients, a fact that Woodcock wanted to avoid because it would mean she knew HCQ was a safe drug. If you recall, Woodcock was instrumental in making the public thing that HCQ was deadly.
See our interview segment on Q Fever treatment here.
‘Epidemic of Fraud’ Fallout: Did the FDA heads know HCQ was safe?

You can read this article and more at our official Broken Truth page. We were recently asked by the French news outlet Francesoir to participate in a rare English language interview with the esteemed Pr Didier Raoult. Dr. Raoult is a world-renowned researcher in the world of medicine with a long and respectable research career. A career that was attacked…
There’s so much scandal and deceit in our health agencies now as they circle the wagons to protect themselves from public scrutiny. As more proof of fraud comes out, expect these same people to turn on each other and begin to provide evidence.
They made you think that tonic water was deadly. And most of you believed it!
Watch Epidemic Of Fraud remastered with better audio right here on BrokenTruth.TV. Exclusively for paid subscribers.

What do you think? Why would the CDC want to remove information about a potential biological weapon with similar symptoms to what we were told was COVID early on? Is it curious that some of the earliest covid outbreaks happened at meat packing facilities?
By the way, did you know that there is a vaccine for Q Fever called QVAX? Do you know what it says about getting the vaccine for Q Fever if you’ve already had the disease? HINT: DON’T DO IT.
It is essential to test for sensitisation to Q fever antigens using Q-VAX® Skin Test in every individual prior to immunisation (see PRECAUTIONS).
CONTRAINDICATIONS
Q-VAX® should not be administered to:
· Persons who have a history of Q fever
· Persons who have been previously vaccinated with Q fever vaccine
· Persons who have a history of likely exposure followed by an illness strongly suggestive of Q fever
· Persons with positive serology for Q fever antibody or a positive Q fever skin test
· Persons with known hypersensitivity to egg proteins or any component of the medicinal product.Those who have a confirmed positive antibody test or a positive skin reaction must not be given Q-VAX® (see PREVACCINATION TESTING).
If the skin test is negative or equivocal and antibodies are present at low titres (reported as a borderline laboratory test result), it cannot be concluded that the subject has adequate protective immunity against Q fever. The low-level presence of antibodies may be non-specific or due to technical factors of the assay. The risk-benefit decision of being vaccinated or not should be individually assessed and discussed with the subject, in order to decide whether potential adverse events following vaccination outweigh the potential risk to that subject from Q fever infection and its associated complications.
It should be noted that a very small number of people may have had Q fever in the past and yet show no response to serological or skin testing. Such persons may have severe reactions to Q-VAX®. For this reason, subjects should be carefully questioned regarding the possibility of previous exposure to Q fever and the duration of such exposure.
Q Fever was relatively novel in the United States. It would have been the perfect weapon to create unexplained outbreaks of pneumonia to drive fear of COVID.
In my FOIA requests to the FDA, the agency had little to know review of the disease at all. Remember, our agencies were too busy covering up their own poor judgment, hiding emails from FOIA, and generating incredible revenue for pharma companies to be bothered with differential diagnoses.
What would it mean if COVID was actually a bacterial weapon and our hospitals refused to treat with antibiotics due to ‘COVID’ protocols?
Q VAX, Q Fever, how about QANON?
When I got "Covid" I had strange bitter taste in my mouth. I don't see such symptom in the Q-Fever symptoms list. If it was the Q-Fever it must have been some kind of an "upgraded" version